
The new evaluation and management coding guidelines took effect on January 1st, 2023. Although they include significant changes for emergency medicine, these changes have already been in effect for outpatient visits for two years. They are intended to simplify requirements and reduce the documentation burden placed on physicians and healthcare professionals. The AMA document detailing all the changes for 2023 can be found here, however it is a 42 page document. This post is an attempt to summarize the guideline changes relevant to practice in the emergency department.
Important changes to keep in mind:
Coding is no longer based on history of present illness (HPI), review of systems (ROS), or physical examination items documented. Instead it is recommended that physicians and other healthcare professionals document what is necessary and helpful for the care of the patient and for colleagues reviewing the medical record.
Instead, coding level is now based solely upon Medical Decision Making (MDM). Although this has always been a part of the emergency medicine chart, it is now the main factor in level of service selection. The American College of Emergency Physicians (ACEP) developed a coding grid for the MDM criteria, specific to emergency medicine. It represents a one page summary of the new requirements. ACEP also published a helpful FAQ on this topic.
What are the medical decision making requirements?
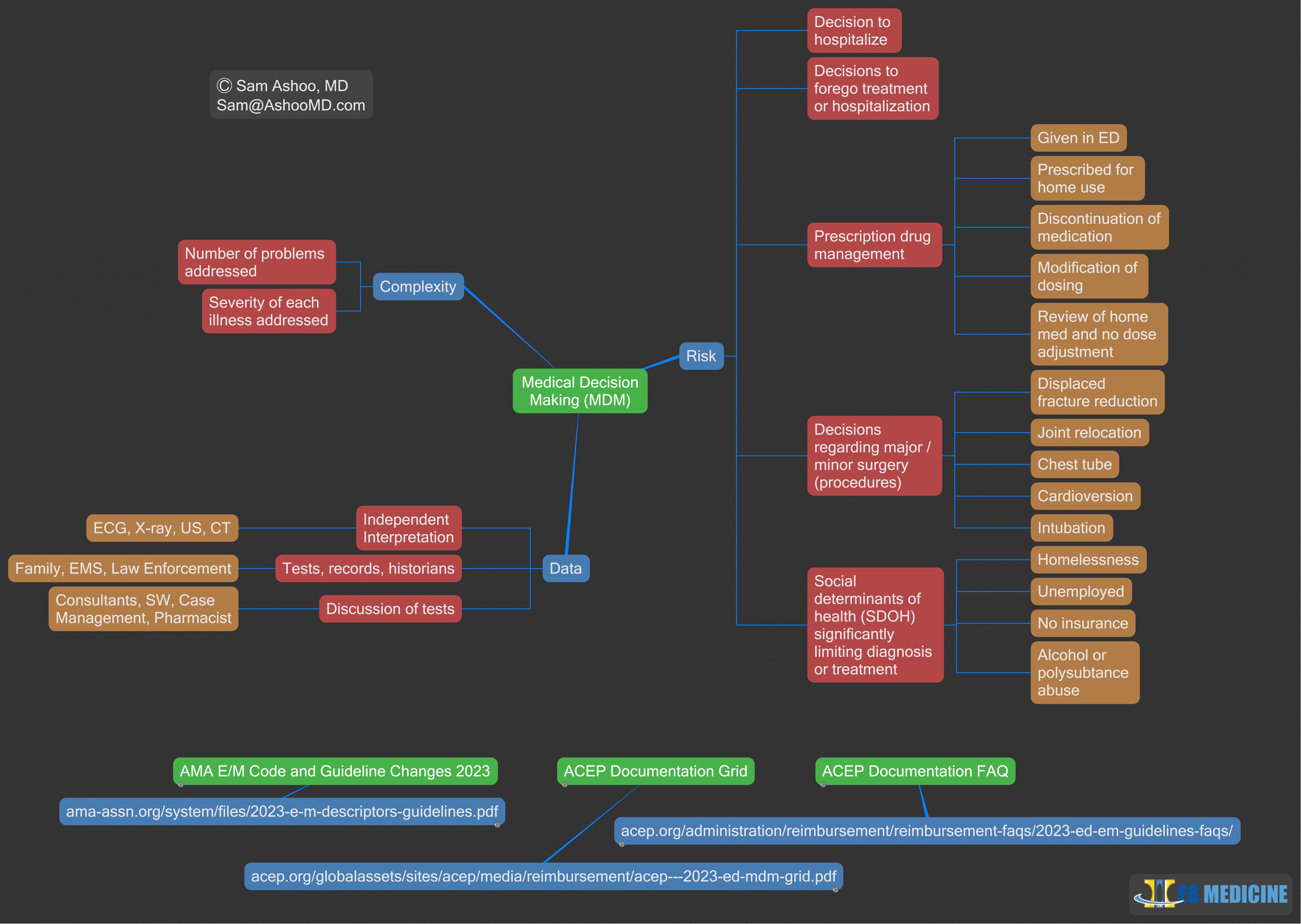
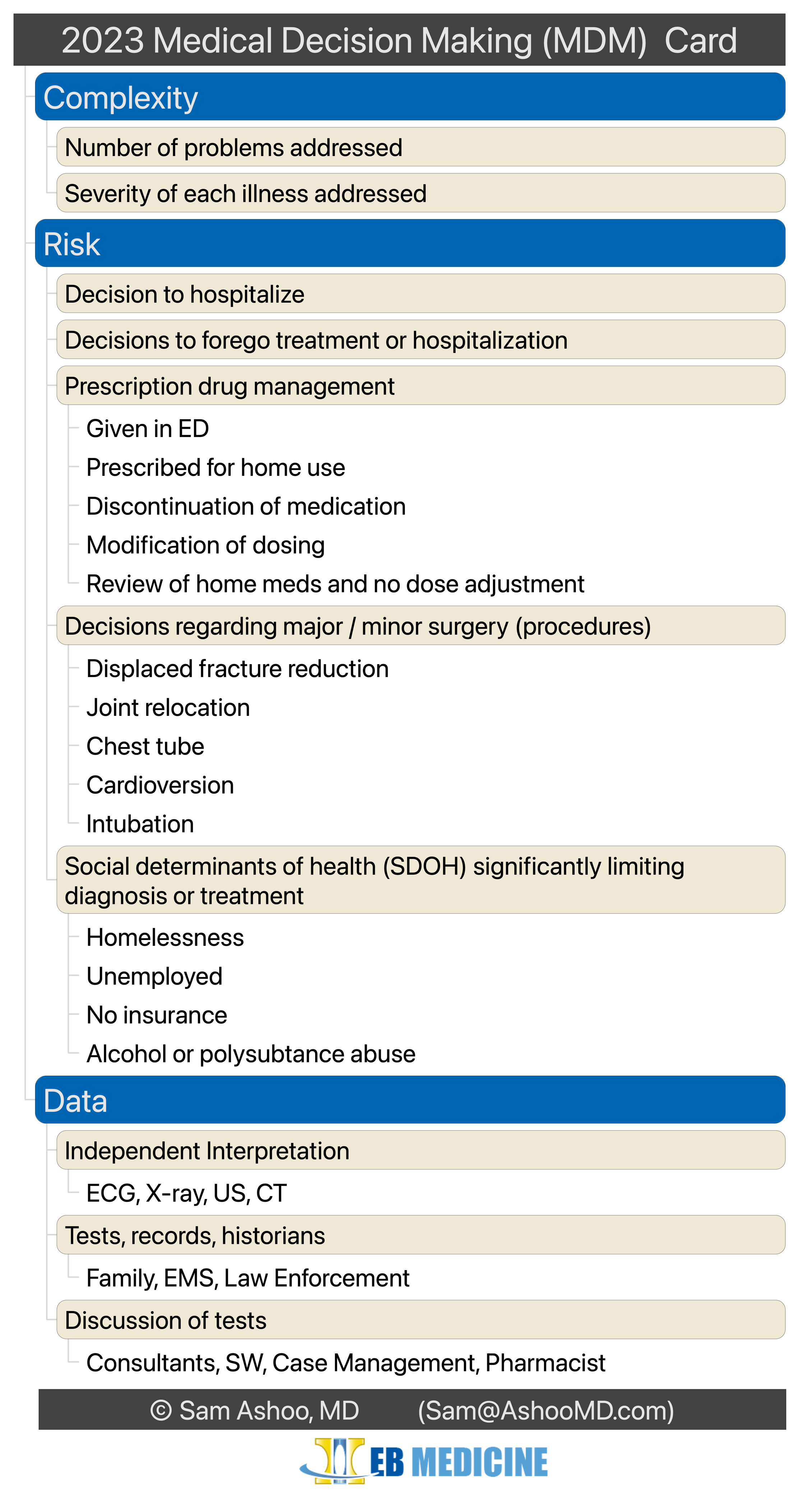
Medical decision making coding is separated into three categories:
- Number and complexity of problems addressed
- Amount and/or complexity of data to be reviewed and analyzed
- Risk of complications and/or morbidity or mortality of patient management
The code selected is based on meeting criteria in 2 out of 3 of these categories. Each category has further clarifications and requirements pertinent to practice in the emergency department.
1. Number and Complexity of Problems Addressed
- A problem does not need to be listed in the diagnosis, but must have been “addressed” to be considered for this category.
- “Addressing” a problem may include considering but not ordering further testing or treatment. Examples include using decision rules to eliminate the need for imaging, considering but withholding medications like antibiotics, or having treatment or diagnostics withheld at patient or family request.
- Since “number” of problems is considered, multiple simple problems addressed may increase the complexity of a case.
- The presence of multiple medical problems (co-morbidities) may be medically relevant, but is not relevant to this category unless they are specifically addressed during the visit.
- The final diagnosis may be a less serious diagnosis than those considered during the evaluation, however it does not change or effect this section’s coding. This means a work up for chest pain may involve advanced imaging to exclude life threatening illnesses but the final diagnosis may be benign.
- Coding for this category includes the number of illnesses addressed and severity of each.
2. Amount and/or Complexity of Data
Three sub-categories exist for the data reviewed:
- Information obtained from tests, records, and historians (patient, family, EMS, etc.).
- “Independent” interpretation of tests, not including those that have a separate CPT code.
- Discussion of tests or interpretations with physicians or qualified health care professionals, including consultation with other-specialty consultants, case management, social work, etc.
3. Risk of Complications, Morbidity, and/or Mortality
Multiple items are included in this category including:
- Decision to hospitalize.
- Decision to forego treatment or hospitalization.
- Prescription drug management including medications given in the ED, prescribed for home use, and/or home medication dosing adjustments.
- Decisions regarding major and minor surgery (procedures) including fracture reduction, joint reduction, chest tube placement, cardioversion, intubation, and more.
- Social determinants of health (SDOH) that significantly limit diagnosis or treatment, including homelessness, unemployment, lack of health insurance, and alcohol or polysubstance abuse.
The images below are meant to serve as a visual representation of the MDM elements. The content is the same, but presented in two formats. They can be downloaded here: Map, Pocket Card . All copyrights are maintained. Permission for redistribution can be obtained by writing me directly at the email address in the images.
{kind=link}
{kind=link}


Disclaimer: This information is purely a summary of the AMA and ACEP publications. It does not constitute financial or coding advice. Specific questions regarding coding and billing should be directed to your coding company or payors.
Last Updated on January 24, 2023
Sam Ashoo, MD, FACEP, is board certified in emergency medicine and clinical informatics. He serves as EB Medicine’s editor-in-chief of interactive clinical pathways and FOAMEd blog, and host of EB Medicine’s EMplify podcast. Follow him below for more…
